CGM for Reactive Hypoglycemia: Complete Guide
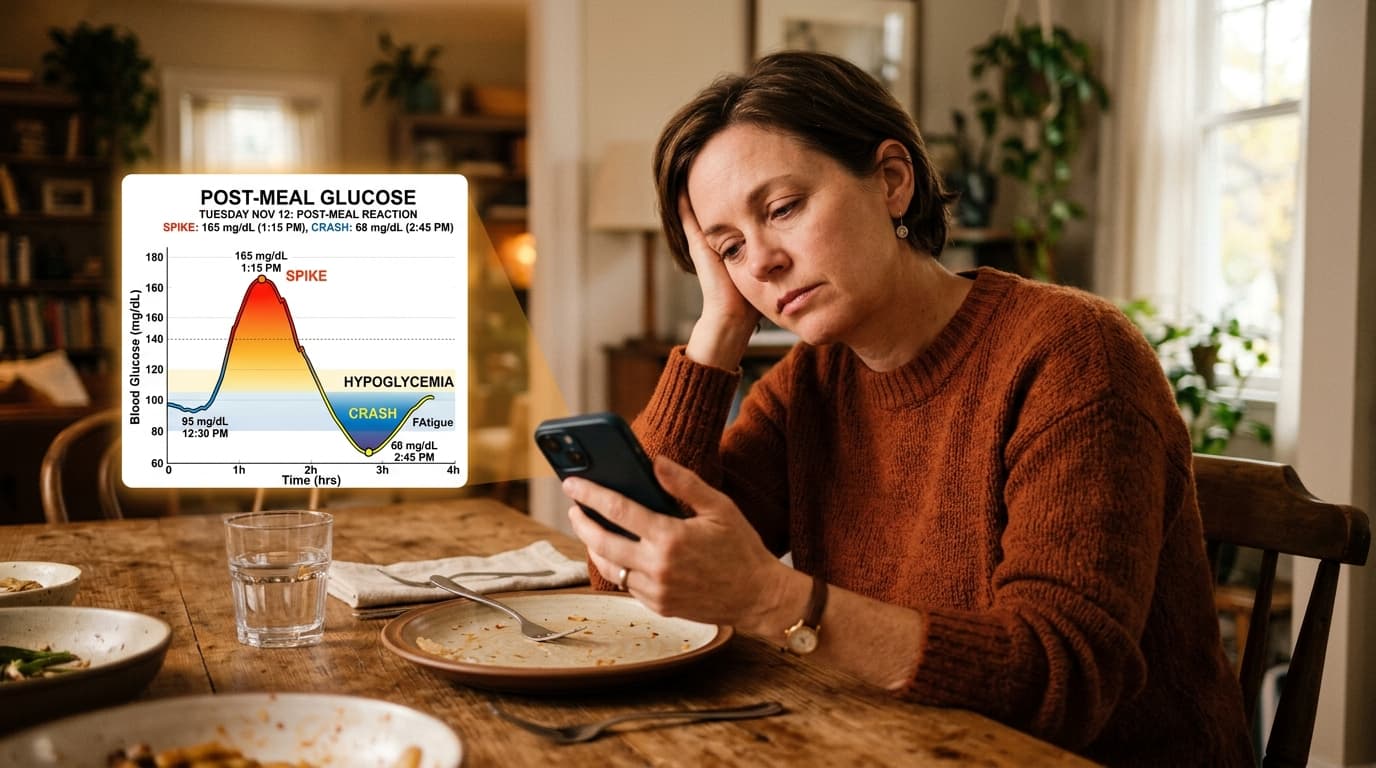
Reactive hypoglycemia (postprandial hypoglycemia) is a condition where blood glucose drops below 70 mg/dL within 2-5 hours after eating, often triggered by high-carbohydrate meals that cause an initial glucose spike followed by an excessive insulin response. Unlike diabetic hypoglycemia, reactive hypoglycemia occurs in people without diabetes and is often underdiagnosed because standard fasting glucose tests miss the postmeal crashes. CGMs are the ideal diagnostic and management tool because they capture the full postprandial glucose curve that single-point blood tests cannot.
Prevalence
Reactive hypoglycemia is estimated to affect 1-9% of the general population, though exact prevalence is difficult to determine because many cases go undiagnosed. It is more common after gastric bypass surgery (occurring in up to 30% of post-bariatric patients).
How Continuous Glucose Monitoring Helps Reactive Hypoglycemia
Reactive hypoglycemia (postprandial hypoglycemia) is uniquely suited for CGM diagnosis and management because the hallmark pattern — a glucose spike followed by a crash below 70 mg/dL, occurring 2 to 5 hours after eating — is invisible to standard diagnostic tests. A fasting glucose test misses it because it only measures baseline levels. An oral glucose tolerance test (OGTT) can detect it but requires a clinic visit and only captures the response to a single glucose load. A continuous glucose monitor captures every postmeal glucose curve, 24 hours a day, for 7 to 15 days — providing dozens of postprandial data points that reveal exactly which meals trigger reactive lows, how severe the drops are, and how long they last. For patients who have undergone gastric bypass surgery (where reactive hypoglycemia occurs in up to 30% of cases), CGM is the most practical long-term monitoring tool.
Key Benefit
Identifies the specific foods and meal compositions that trigger postmeal glucose crashes, allowing targeted dietary changes that eliminate reactive hypoglycemic episodes in up to 78% of patients.
Recommended CGM Devices
Because reactive hypoglycemia occurs in non-diabetic individuals, over-the-counter CGMs are the primary option. The Dexcom Stelo at $99/month provides the familiar Dexcom interface and app ecosystem without a prescription. The Abbott Lingo at $49/month is the most affordable choice for identifying postmeal crash patterns. For patients who want guided interpretation of their glucose curves, Nutrisense or Levels subscription services include dietitian coaching that can help translate CGM data into meal-composition changes (adding protein and fat to high-carb meals, reducing simple sugars). Some endocrinologists prescribe a 14-day diagnostic CGM trial using a FreeStyle Libre 3, which may be partially covered by insurance if the clinical indication is documented.
Insurance Coverage
Insurance rarely covers CGMs for reactive hypoglycemia since it is not a diabetes diagnosis. Over-the-counter CGMs like Dexcom Stelo and Abbott Lingo are the most accessible options, available without a prescription at $49-99 per month. Some endocrinologists can prescribe a diagnostic CGM trial (typically 14 days) that may be covered if the clinical indication is documented.
Insurance coverage for CGMs in reactive hypoglycemia is limited because it is not classified as diabetes. Most patients will need to use OTC CGMs ($49-99/month) or pay out of pocket. However, some endocrinologists can prescribe a short-term diagnostic CGM trial that may be partially covered if the documentation includes symptoms consistent with hypoglycemia, a referral to endocrinology, and evidence that standard testing (OGTT) has been inconclusive. HSA and FSA accounts can be used for CGM purchases. For post-bariatric patients with documented reactive hypoglycemia, insurance coverage is more likely because the condition is a recognized surgical complication.
Clinical Evidence
A 2020 study in the Journal of the Endocrine Society found that CGM identified reactive hypoglycemia in 32% of patients with unexplained postprandial symptoms who had normal oral glucose tolerance tests. Research published in Nutrients (2022) demonstrated that CGM-guided dietary modifications (reducing refined carbohydrates, adding protein/fat to meals) eliminated reactive hypoglycemic episodes in 78% of patients within 4 weeks. The International Hypoglycaemia Study Group recommends CGM as the gold standard for diagnosing and monitoring non-diabetic hypoglycemia.
A 2020 study in the Journal of the Endocrine Society found that CGM identified reactive hypoglycemia in 32% of patients with unexplained postprandial symptoms who had normal OGTTs — demonstrating that CGM is more sensitive than standard diagnostic testing. Research in Nutrients (2022) showed that CGM-guided dietary modifications eliminated reactive episodes in 78% of patients within 4 weeks. A 2023 study in Obesity Surgery found that CGM monitoring in post-bariatric patients detected an average of 2.3 hypoglycemic episodes per day that were previously unrecognized. The International Hypoglycaemia Study Group recommends CGM as the gold standard for diagnosing and monitoring non-diabetic hypoglycemia.